You’ve probably heard someone ask you a would you rather question once in your life, right? How did you answer back? Life is full of options to take, and we have to make the best choices when faced with situations.
Sometimes, these choices are not as favorable, but we make them work. And how we wish that our life, work, and relationships are easy as making a “this or that” choice. Wouldn’t that be more manageable?
In this episode, we will be taking a break from our usual topics and let a little loose in this one. Today we will ask our “Would You Rather” questions nurse edition and share our thoughts about them.
We hope you find this episode entertaining as much as we enjoyed answering these questions. Check it out!
Would You Rather: Nursing Edition Questions
Would you rather do admission or discharge?
Would you rather work a 24-hour shift or oversleep and be late for your shift?
Would you rather be punched in the face or spit in the mouth?
Would you rather have a rude, ungrateful patient or a patient with a difficult helicopter parent/family member?
Would you rather be a nurse on a cruise ship or a nurse at a music festival?
Would you rather have co-workers love you and your manager hate you? Or have your co-workers hate you and your manager love you?
Would you rather be ignorant and blissful or smart and never happy?
Would you rather have a C. Diff vs. GI Bleed patient?
Would you rather do the laundry or the dishes for the hospital?
Would you rather be the strongest man on earth or the smartest man on earth?
Would you rather get shit slapped in the face while trying to subdue a psych patient or have to give a bed bath to a patient with bed bugs?
Would you rather love your hospital, pay, co-workers and managers and hate your city and your life outside of work? Or would you rather hate your hospital, pay, co-workers and managers but love your city and life outside of work?
Would you rather have spilled urine on your pants or trach sputum on your shirt?
Would you rather have vomit in your hair and mouth? Or poop down your shirt?
Would you rather live the rest of your life as a Buddhist monk or be followed continuously by the paparazzi?
Join us as we answer these questions! Watch the full Episode 160 by clicking here 👇
TIMESTAMP:
00:00 Intro 00:53 Plugs 02:57 Episode Intro 03:42 Admission or discharge? 05:12 Work a 24-hour shift or oversleep and be late for your shift? 06:24 Redo your nursing school program or high school? 07:50 Punched in the face or spit in the mouth? 09:14 A rude, ungrateful patient or a patient with a difficult helicopter parent/family member? 11:05 A nurse on a cruise ship or a nurse at a music festival? 12:54 Have co-workers love you and your manager hated you? Or have your co-workers hate you and your manager love you? 14:14 Ignorant and blissful or smart and never happy? 16:26 C. Diff vs. GI Bleed patient? 18:00 Do the laundry or the dishes for the hospital? 19:33 The strongest man on earth or the smartest man on earth? 20:16 Get shit slapped in the face while trying to subdue a psych patient or have to give a bed bath to a patient with bed bugs? 22:49 Love your hospital, pay, co-workers and managers and hate your city and your life outside of work? Or would you rather hate your hospital, pay, co-workers and managers but love your city and life outside of work? 24:11 Have spilled urine on your pants or trach sputum on your shirt? 26:02 Have vomit in your hair and mouth? Or poop down your shirt? 28:25 Live the rest of your life as a Buddhist monk or be followed continuously by the paparazzi?
Looking for more nursing and travel nursing information? Check out these helpful links!
Soil degradation and retrogression are two regressive evolution processes associated with the loss of equilibrium of stable soil. So we think that soil degradation and human demise are the end results if this kind of soil condition continues.
Retrogression is primarily due to soil erosion and corresponds to a phenomenon where succession reverts the land to its natural physical state.
Soil is lost due to erosion from wind and water— for example, rivers washing upland or wind blowing dirt away.
Degradation is due to the replacement of primary plant communities by secondary communities. This replacement modifies the humus composition and amount and affects the formation of the soil.
It is directly related to human activity.
What is Soil?
The definition of soil is “The unconsolidated mineral or organic material on the immediate surface of the Earth that serves as a natural medium for the growth of land plants.” [1].
Soil is one of the world’s most needed resources. We think about animals and this idea of going “plant only” but don’t understand that this might not be the best thing for ourselves and our environment.
When was the last time, if ever, we thought about soil health? It isn’t something that comes to mind as necessary, even when we think about human survival. Ask yourself what do humans need to survive? Water and food.
Water is found in natural bodies of water, but where do you get food from? Soil is required for plants, animals require plants, and as humans, we need to eat animals and plants.
The Soil Profile
As soils develop over time, layers (or horizons) form a soil profile. Most soil profiles cover the earth as two main layers—topsoil and subsoil.
Soil horizons are the layers in the soil as you move down the soil profile. A soil profile may have soil horizons that are easy or difficult to distinguish. [2]
Most soils exhibit 3 main horizons:
A horizon: humus-rich topsoil where nutrient, organic matter, and biological activity are highest (i.e., most plant roots, earthworms, insects, and micro-organisms are active). The A horizon is usually darker than other horizons because of the organic materials.
B horizon: clay-rich subsoil that is often less fertile than the topsoil but holds more moisture. It generally has a lighter color and less biological activity than the A horizon. Texture may be heavier than the A horizon too.
C horizon: underlying weathered rock (from which the A and B horizons form).
Some soils also have an O horizon, mainly consisting of plant litter accumulated on the soil surface.
The properties of horizons are used to distinguish between soils and determine land-use potential.
What is in the soil we use?
Soil contains air, water, minerals, and plant and animal matter, both living and dead. These soil components fall into two categories.
In the first category are biotic factors—all the living and once-living things in the soil, such as plants and insects.
The second category consists of abiotic factors, including all nonliving things—minerals, water, and air.
The most common minerals found in soil that support plant growth are phosphorus, potassium, and nitrogen gas. Other less common minerals include calcium, magnesium, and sulfur. The biotic and abiotic factors in the soil make up the soil’s composition.
Minerals
The most significant component of soil is its minerals, accounting for about 45% of its volume. The most common ones are phosphorus, potassium, and nitrogen. While the less common ones are magnesium, calcium, and sulfur.
Water
Water is the second essential component of soil. It makes up approximately 2% to 50% of the soil volume. It is vital for transporting nutrients to growing plants and soil organisms and facilitating biological and chemical decomposition. Soil water availability is the capacity of a particular soil to hold water available for plant use.
Organic Material
Organic matter is the next primary component found in soils at levels of approximately 1% to 5%. This matter is derived from dead plants and animals and has a high capacity to hold onto and provide the essential elements and water for plant growth. An organic matter has a tall “plant available” water-holding ability and CEC, which can enhance the growth potential of soils.
Gas
Gases and air are the following essential component of soil. They make up approximately 2% to 50% of the soil volume. Oxygen is necessary for root and microbe respiration, which helps support plant growth.
Carbon dioxide and nitrogen gas are also crucial for belowground plant functions like nitrogen-fixing bacteria. If soils remain waterlogged (where gas is displaced by excess water), it can prevent root gas exchange, leading to plant death, a common concern after floods.
Microorganisms
Microorganisms are the final fundamental element of soils. They are present in the ground in high numbers but make up less than 1% of the soil volume. An estimate is that, one thimble full of topsoil hols more than 200,000 microbial organisms.
Earthworms and nematodes are the largest organisms found in soil. The smallest are algae, fungi, actinomycetes, and bacteria. Microorganisms are the primary decomposers of raw organic matter. Many decomposers eat up organic matter, water, and air. This is to recycle natural organic matter into humus, rich in plant nutrients [3].
Nutrient Depleted Soil
Nearly 99 percent of the world’s daily calorie intake can be traced back to the soil. The plants and animals we eat require soil to grow. Soil is vital for human survival, yet modern farming and agricultural practices quickly destroy it.
Worldwide, one-third of the Earth’s soil is at least moderately degraded, and over half of the land used for agriculture has some soil degradation.
Due to intense, mismanaged farming, soil nutrients are declining.
Nitrogen stores have decreased by 42 percent
Phosphorus by 27 percent
Sulfur by 33 percent.
Plants require these nutrients for photosynthesis, enzymes, protein synthesis, and more to grow optimally.
As a result of declining soil fertility and selective breeding, the nutritional contents of some fruits, vegetables, and grains have also been compromised.
In a 2004 study using USDA data, 43 garden crops were analyzed to compare nutritional content in 1950 versus 1999. Some nutrients were unchanged, but calcium, phosphorus, iron, riboflavin, and vitamin C were lower in 1999 compared to 1950, ranging from a 6 percent to 38 percent drop [4].
The protein content in corn declined from 30 percent to 50 percent from 1920 to 2001, while the starch content increased [5].
The magnesium content of vegetables and wheat has declined by up to 25 percent. There are trace minerals in vegetable crops. Minerals like manganese, zinc, copper, and nickel, have decreased over the last decades. Toxic minerals like aluminum, lead, and cadmium have increased [6].
The current agriculture methods produce higher yields but deplete and erode soils. Currently, industrial agriculture is destroying the soil. It is being destroyed at 100 to 1,000 times the rate where it is replenished. It is according to the United Nations estimates. According to their report, we only have 60 years left of harvest in many farming regions.
What contributes to soil degradation and human demise?
Monoculture
Many industrial farms grow one single crop, year after year after year. This kind of practice depletes the soil and contributes to carbon loss and soil erosion. Agricultural farms must include perennial crops, legumes, and forages in rotation. This returns the organic matter in the soil, prevents decay, and replenishes nutrients.
For example, legume crop residues can be converted into nitrogen by soil bacteria, reducing the need for synthetic nitrogen-based fertilizers.
Additionally, monocropping can threaten food security. With a single crop species on millions of acres, one disease could potentially wipe out an entire food system.
Synthetic Fertilizers
Instead of using organic fertilizers, including crop rotations, cover crops, and manure, modern farms require massive amounts of synthetic fertilizers to grow crops continually.
Nitrogen-based fertilizer production has increased by 9.5-fold since 1960. Fertilizer production consumes fossil fuels in a very energy-intensive process, with non-negligible environmental consequences.
Not all the fertilizers applied are used up by the crops. Fifty percent or more of the nitrogen leaches into the environment. Many inorganic fertilizers destroy soil microbes that have roles in soil homeostasis.
Ammonia, nitrate, and other nitrogen residues make their way to groundwater, rivers, and eventually, the ocean. They reduce oxygen levels, increase algae growth, and damage or death to aquatic life.
Tillage-Based Farming
Farms today till fields to remove crop residues, flatten the land, and generally mix up the topsoil. However, tilling reduces microbe populations in the soil, promotes soil erosion, and releases greenhouse gases. Today, 93 percent of the world’s cropland uses tilling-based methods for production.
Herbicides, Pesticides, and Fungicides
Herbicides, pesticides, and fungicides can help increase crop yield. By keeping weeds and harmful organisms under control. The benefits come with costs. And when this problem continues soil degradation and human demise is going to be our future.
Additionally, pesticide residues make their way into water systems and food. Many health problems have been linked to pesticide exposure, including asthma, neurological issues, and even cancer.
The most well-known herbicide is glyphosate, which is applied to crops for hundreds of millions of pounds each year. Glyphosate has profound environmental and health consequences, covered in this article.
Mismanaged Grazing
Cows and other ruminants have the unique ability to convert grasses and other plants that are inedible for humans into nutrient-dense, edible animal products.
Best practices dictate that ruminants should rotate among different fields, allowing sections of grass to rest and regrow.
But when cows graze on the same land as in many conventional farms, it contributes to soil erosion. It lowers soil carbon reserves. Overgrazing contributed to the loss of about one-fifth of the world’s grasslands
Unfortunately, the importance of ruminant animals has been almost forgotten. Due to rocky terrain, hills, and climate, much of the world’s land isn’t even conducive for growing crops.
In contrast, cows, sheep, and goats can often thrive on these marginal lands. Yet these areas aren’t being fully utilized to raise ruminants for food and to sequester carbon properly. Instead, we have concentrated animal feeding operations, or CAFO, where grazing is limited, cows are fed grain residues from an outlying farm.
Unity Between the Human Body and Soil
Our body is from soil and water. Without those 2, there is minimal to no possibility of human life. The quality of soil impacts the quality of our physical, spiritual, and mental selves.
Think about evolution or spirituality – if we stem from one at one point. We were the soil or some component of it, so now we are forever bound to the ground. In that soil, there is life, and from that life, there comes bigger life. Not only does it help in a physical sense but spiritual sense too.
When you eat bad food, you feel sick. This sickness manifests physically, mentally, and even spiritually. If you have food poisoning, how do you move? How does it then change your thinking? How does it influence your beliefs? Soil connects to us.
We are treating soil like some infinite disposable thing. Now take a look at how some humans treat other humans? How toxic people in power treat people below them.
The word human stems from the word “humus” in Latin, which means soil. As translated to “living soil” – as in the ground needed for growth. Less and less nutrient-dense foods can lead to the shunting of human growth and function.
To learn more about soil degradation and human demise, watch the full Episode 96 in this video 👇
SHOW NOTES:
00:00 Intro 00:52 Plugs 02:08 Soil Degradation and Human Demise 07:25 What is soil? 09:54 The layers of soil 12:35 The essential life-building blocks in soil 16:43 Nutrient Depleted Soil 20:37 Soil Erosion: Monoculture 21:58 Soil Erosion: Synthetic Fertilizers 24:21 Soil Erosion: Tillage-Based Farming 25:19 Soil Erosion: Herbicides, Pesticides, and Fungicides 27:35 Soil Erosion: Mismanaged Grazing 30:14 Unity Between the Human Body and Soil 35:20 Wrapping up the episode
Being an ICU nurse is not for the weak. Nurses are witnesses to a patient’s most vulnerable time of their life. And for us nurses, it is a blessing to be a part of that.
Working as an ICU nurse taught us many things workwise and experiencing the negative and positive impacts of being one.
In this episode, we will talk about the pros and cons of being an ICU nurse, share our experiences and inspire those interested in becoming one in the future.
How we became ICU nurses started at the hospital when we were still new nurses ourselves. In Matt’s case, becoming an ICU nurse was easy – he was inspired by an ICU nurse who showed him what’s it like to handle a situation, which left him with a good impression.
Moments like this are rare because when you are a new grad nurse, you often get assigned to one area where you get to work for a year or so and not be able to explore other areas in nursing.
Being an ICU nurse is interesting because we get involved in the littlest thing with our patients. Every orifice, drop, whatever comes in or out – we know it all. It’s like doing science and history at work.
We all get to see where our patient came from, their present condition, and working ways to help them be better in the future.
Nurses as Role Models
Imagine if Matt’s interaction with that ICU nurse was a negative one. Perhaps he wouldn’t even try exploring the ICU or being an ICU nurse.
As nurses, we have to be good examples to people because our actions can either impress or distress others who have the potential to be good nurses someday.
That said, here are the pros and cons of being an intensive care unit nurse:
Pros of Being an ICU Nurse
Collaboration with other healthcare professionals to help the patient as a team – you get to see the whole picture of the situation.
Easy access to the medical team. Intensivists vs hospitalists.
Larger autonomy and scope of practice – nurses can practice using their critical thinking skills to help the patients.
Great career progression to reach CCRN or even management.
2:1 and 1:1 patient ratios.
Learning curve – learning to prioritize/critical thinking.
Cons of Being an ICU Nurse
We get the worst of the worst, like ETOH withdrawals – you want to help, but sometimes the situation can be stressful because of unruly patients.
Crashing patients with a lot of drip management – is the opposite of the “worst of the worst”. Your patient keeps crashing, no matter how much you try to help them.
High stress – we don’t respond stressed out all the time, but the tasks/care we give is a constant level of stress. It can be exhausting by the end of the day.
Difficult dealing with family, decision making & family drama. – an emotional strain that can put you in a tough spot. You are the response team.
Physical labor – this is not just ICU. We are in charge of full care usually because patients in our unit don’t participate in our care. There’s a possibility of workplace injury.
Nasty wounds and messy patients – you get to clean up the body fluids that come out of your patients, like sputum, drool, urine, feces, etc. If you are easily squeamish, this is not the place for you.
Loss of patient care – higher mortality in the ICU. Dealing with the hardships. How to cope.
No extra pay – some healthcare facilities don’t pay ICU nurses much, given all the responsibilities that they have.
How did C19 affect the ICU as far as workload?
Usually, an intensive care unit is limited only to two patients, but hospitals have been flooded with critical patients since the pandemic broke out.
More patients are sent to the ICU nowadays, and nurses’ role has tripled over time. From monitoring patients to dealing with the loss, and helping families, it’s a tough job, to be honest.
The idea that nurses are navigating new territories adds to the emotional stress of their work, more critically ill patients, dying patients, and dealing with the emotions of the families who just lost a loved one. It is a stressful time to be an ICU nurse.
But then again, it is something worth taking because of how rewarding our job is.
How to know if ICU Nursing is right for you?
Being an ICU nurse is not for everyone. It’s a tough job, to be honest. But as you grow with the job, your perspective in life changes too.
There’s no specific personality or knowledge to being an ICU nurse. You don’t need to be perfect for the job because you will never know if it is the right job for you unless you give it a try.
As you go, you learn with experience. We all learned from experience in nursing school and now in real life. Nursing school was hard, but you made it.
The same goes with ICU nursing, it may be hard from the beginning, but that doesn’t mean it won’t help you grow in your career.
Of course, you have an option to give it a try and see where it goes. As a nurse, there are so many fields of nursing that you can explore.
Maybe ICU nursing is your thing, maybe not. And that’s fine too.
The important thing is that you know where your heart is in this profession, so you can excel at the work you have chosen.
In Closing
There are so many ways being a nurse can take you. It would be best if you didn’t waste your time doing something you are not happy with.
Our time as ICU nurses has been a real blessing. It taught us wisdom and humbled us in many ways. We wouldn’t want to change that.
Of course, we enjoy being travel nurses, but the lessons we have learned as ICU nurses will always have a special place in our lives.
Hopefully, you can also find that as you embrace being an ICU nurse in the future.
Learn more about the pros and cons of being an ICU Nurse in this full episode. Click here 👇👇👇
TIMESTAMPS:
00:00 Intro 00:55 Plugs 02:36 Episode Introduction 07:06 Pro: Health Care Team Collaboration 10:38 Pro: Access to other medical teams 12:40 Pro: Larger autonomy and scope of practice 15:03 Pro: Great career progression 15:52 Pro: Patient ratio 18:36 Pro: More on the critical task 19:59 Con: ETOH or unruly patients 21:20 Con: Crashing patients 23:51 Con: High stress 27:12 Con: Physical Labor 30:59 Con: Dealing with nasty wounds, blood, sputum, etc. 32:16 Con: Compensation 34:16 ICU is for you if… 36:08 Wrapping up the episode
Looking for more nursing and travel nursing information? Check out these helpful links!
Muscle growth and hypertrophy are essential when you want to stay fit. Everyone has muscles, but many want them to be a bit bigger. Did you know there are over 600 muscles in your body?
Muscles are responsible for actions like movement, digestion, circulation, and respiration. There are different muscles for each job in the body.
Injuries, diseases, and various disorders affect the way your muscles function. These issues can be muscle pain spasms or more severe, like paralysis and cardiomyopathy.
Living a healthy lifestyle through good nutrition and adequate exercise prevents early deterioration of muscle and function and improves endurance, size, and strength.
Muscles
Muscles’ function is to contract and relax. It doesn’t matter if that muscle is voluntary or involuntary. It is going to contract in one-way shape, or another.
The somatic nervous system is responsible for the voluntary movement of skeletal muscle, while the autonomic nervous system is responsible for involuntary action like that of smooth muscle[1].
3 Different Types of Muscle Tissue
There are three different types of muscle tissues. Each type of muscle also functions differently within different areas of the body. These are:
Skeletal: As part of the musculoskeletal system, these muscles work with your bones, tendons, and ligaments. Tendons attach skeletal muscles to bones all over your body. Together, they support the weight of your body and help you move. You control these voluntary muscles.
Some muscle fibers contract quickly and use short bursts of energy (fast-twitch muscles). Others move slowly, such as your back muscles that help with posture.
Cardiac: These muscles line the heart walls. They help your heart pump blood that travels through your cardiovascular system. You don’t control cardiac muscles. The heart tells them when to contract.
Smooth: These muscles line the insides of organs such as the bladder, stomach, and intestines. Smooth muscles play an essential role in many-body systems. These include the female reproductive system, male reproductive system, urinary system, and respiratory system.
Different types of muscles work without you having to think about them. They do essential jobs like moving waste through your intestines and helping your lungs expand when you breathe.
Skeletal Muscle
Skeletal muscles consist of flexible muscle fibers that range from less than half an inch to just over three inches in diameter. These fibers usually span the length of the muscle.
The fibers contract or tighten, allowing the muscles to move bones so you can perform lots of different movements.
Skeletal Muscles Structure
Each muscle can contain thousands of fibers. Different types of sheaths, or coverings, surround the fibers:
Epimysium: The outermost layer of tissue surrounding the entire muscle.
Perimysium: The middle layer surrounding bundles of muscle fibers.
Endomysium: The innermost layer surrounding individual muscle fibers.
Actin and myosin are both proteins that are found in every type of muscle tissue. Thick myosin filaments and thin actin filaments work together to generate muscle contractions and movement.
Myosin is a type of molecular motor that converts chemical energy released from ATP into mechanical energy.
This mechanical energy is then used to pull the actin filaments along, causing muscle fibers to contract and, thus, generate movement.
What does skeletal muscle look like?
Skeletal muscle fibers are red and white. They look striated or striped, so they’re often called striated muscles. Cardiac muscles are also striated, but smooth muscles aren’t.
How healthy is skeletal muscle?
Although skeletal muscles typically make up roughly 35% of your body weight, this can vary from person to person. Men have about 36% more skeletal muscle mass than women.
People who are tall or overweight also tend to have higher muscle mass. Muscle mass decreases with age in both men and women.
Hypertrophy
In simple terms, hypertrophy just means “to make bigger.” It is the opposite of atrophy which is to make it smaller. When we talk about hypertrophy in muscles, we mean muscle growth.
Muscle growth and hypertrophy is the primary goal of why people work out and train.
When you talk about muscular hypertrophy, it is different from just gaining strength. Although with hypertrophy comes more strength, it is a different concept and different mode of work than strength training [2].
Hypertrophy is done to increase the size of a muscle
Strengthening is done to increase the ability to produce force
2 Different Types of Hypertrophy
1. Myofibrillar hypertrophy
This type of muscular hypertrophy involves increasing the number of protein filament bundles known as myofibrils.
Myofibrils help the muscle contract and relax. Increasing myofibrils boost muscular strength. With myofibril hypertrophy, the muscle also becomes denser [3].
Growth of muscle contraction parts.
2. Sarcoplasmic hypertrophy
You can also increase the volume of fluid within the muscle. This is called sarcoplasmic hypertrophy. The fluid provides the energy the muscle needs during weight training.
Similar to how adding water to a balloon makes the balloon grow, more fluid in the muscle makes it look bigger [4].
Increased muscle glycogen storage.
How to Build Muscle?
There are many ways to muscle growth and hypertrophy and strengthen muscle, but we want to focus on how to maximize hypertrophy.
1. Diet and Sleep
You need proper fuel and rest to build muscle. There has always been a debate between carbs, proteins, and fats. With so many diets out there, you should not solely rely on one of them.
The main thing to always keep in mind when it comes to the human diet is that we need all the macronutrients.
It would help if you ate carbs, proteins, and fats. Neglecting any one of those will directly impact not only your muscle growth but your overall health.
Proteins get broken down into amino acids, which are the building blocks of all our cells. Carbs are your body’s primary source of fuel.
Fats are required for hormone function. Many studies show the benefit of eating a higher amount of protein when trying to build muscle.
Research indicates that achieving muscle hypertrophy requires balancing muscle protein synthesis and muscle protein breakdown.
Additionally, consuming protein within 24 hours of weight training can provide a positive net balance.
This net balance supports muscle growth. Follow your workouts with higher protein meals or shakes to give the body the nutrients to achieve maximum hypertrophy.
Carbs are beneficial for:
Carbs prevent muscle weakness
It can prevent muscle degradation
Carbs help muscles recover from exercise
Recommended Protein Intake for Muscle Growth and Hypertrophy
Individuals in Energy Balance
Consume ~0.4 g/kg body mass (i.e., 0.24 plus 0.06 with protein added to account for the influence of other macronutrients in meals and protein quality), to maximally stimulate muscle protein synthesis (MPS) following a period of rest or exhaustive resistance exercise.
Spacing protein-containing meals ~3–5 h throughout the day maximizes MPS rates over the course of a 12 h (i.e., waking) period.
Practice pre-sleep protein ingestion (1–3 h prior to sleep) to offset declines in MPS that would occur during an overnight fasting period.
To maximize muscle protein accretion with resistance exercise, daily protein intakes should be ~1.6 g/kg/day and up to 2.2 g/kg/day. This intake can be achieved by ingesting 3 meals, each containing ~0.53 g/kg protein, or 4 meals containing ~0.4g/kg protein.
Individuals in Energy Restriction
Daily protein requirements are greater than they are during periods of energy balance to promote the maintenance or increase in lean body mass.
Resistance exercise should be performed during energy restriction to promote the retention of lean body mass if desired.
For athletes cutting weight over an extended period, high-quality protein sources such as whey and casein, or a blend of each, should be chosen to optimize appetite control and ensure dietary compliance.
Protein intakes of ~2.3–3.1 g/kg/day have been advocated to promote leaner body mass retention during weight loss. Exercise-naive adults who have a more significant body fat percentage should aim to achieve the lower end of this range. However, leaner individuals with resistance-training experience who are more vulnerable to losing lean body mass during energy restriction should aim for the higher end of this range[5].
2. Exercise
With exercise, muscle growth and hypertrophy are induced. What causes it is “as calcium is released in higher quantities with each contraction induced by the neuron, calcium binds to calmodulin. It activates calmodulin kinases (CaMKs), and in turn, activates Akt, which activates protein synthesis via mTOR and the inhibition of glycogen synthase pathways.”
Muscle growth is achieved when a combination of things occurs: muscle damage and repair, mechanical tension through stretch and force, and the build-up of metabolites like lactate, hydrogen ions, creatine, and others.
Metabolite accumulation can occur as lactate, hydrogen ions (lowering pH), and phosphate molecules accumulate within the cell.
The collection of these, and likely others (like creatine), metabolites in the cell shows an increased expression of Insulin Growth Factor-1 (IGF-1).
This increases the proliferation of satellite cells and increases protein synthesis via the Akt pathway.
Also, the increase in growth hormone (GH) further increases the release of IGF and release of Interleukin-6 (IL-6) for different effects on satellite cell recruitment.
How Muscles Work During Exercise
To be able to return for another bout of exercise, the trauma to the muscle leads the cell to release calcium (likely due to damage to the sarcoplasmic reticulum) into the surrounding extracellular area; this release of calcium leads to the activation of an immune response.
As soon as one hour after this event, neutrophils go through phagocytosis and clean up the debris of dislodged and broken organelle proteins caused by the stress put on the myocyte.
24-48 hours after myocyte damage, macrophages are the dominant immune cells finishing phagocytosis and releasing cytokines and growth factors to activate other immune clean-up cells and the repair process.
These cytokines, Interleukin-1, 6, and tumor necrosis factor (TNF), are the regulators of inflammatory response and communicate more or less the need for further necrosis and inflammation between immune cells.
Growth factors such as growth hormone (HGH), insulin-like growth factor (IGF), fibroblast growth factor (FGF), and hepatocyte growth factor (HGF) are released to begin the repair process.
Main Concepts and Strategies When Exercising
To accomplish muscle growth and hypertrophy, you have to induce some kind of physical activity. The main concepts and strategies to think about when creating a program or just in exercise are:
1. Engage in strength training regularly.
You can’t just work a muscle once and expect it to grow. It needs to be stressed repeatedly over time.
Resistance training at least three times per week can provide the tension necessary for the muscle to adapt and grow.
Constantly doing the same exercise over again is an excellent place to start. Over time repeating the same workout does lead to fewer results, so it is essential to switch up the routine.
2. Increase resistance over time.
Starting with lighter weights gives the muscle time to adjust to a new weight training program. But once that weight becomes easy to lift, it needs to be increased if the goal is hypertrophy.
The general rule is to increase your weight by about 5-10% to prevent injury.
3. Aim to overload the muscle or muscle group.
If you walk out of your weight training sessions feeling as if you could go through the sets and reps again, you’re not overloading your muscle enough.
While you don’t want to go to the point of pain, growing muscle requires a certain level of overload. During your workout, aim to push your muscle as much as possible while still being safe.
4. Lift heavy for higher reps.
A hypertrophy workout involves lifting fairly heavy weights. You also want to shoot for higher reps than if your goal was strength. Again, you have to overload the muscles to a certain extent if you want them to grow [6].
5. Sets and repetitions.
Start muscle growth and hypertrophy with two to three sets of ten to 15 reps, completing repetitions at a manageable but challenging weight.
So if you are doing three sets of 12 repetitions, the weight you use should be heavy enough that you cannot do more than 12 reps but not so heavy that you cannot get to 12.
If you know your one-rep max and have the basics of working out, you should be looking to lift between 65%-75% of your 1RM for eight to 12 reps for three to six sets.
6. Reduce your rest periods.
The rest time between sets changes based on whether the goal is to increase muscle size or strength.
The recommended rest period is generally between two and five minutes for strength increases.
This period is shortened to 30 to 90 seconds to increase muscle size.
7. Allow adequate time for muscle recovery.
Getting enough recovery time is critical to building bigger muscles. It is during this recovery that muscle damage is repaired.
Therefore, if you don’t allow enough time for this repair to occur, not only will muscles not reach their maximum size, but you also risk injuring them.
Allow 24 to 48 hours before working for the same muscle group again [7].
Muscle Soreness
Many people have sore muscles after working out. The soreness results from tiny tears (microtears) occurring when you put stress on a muscle.
Usually, muscle soreness sets in a day or two after vigorous exercise. This condition is why providers call this condition delayed onset muscle soreness (DOMS).
The muscle tissue becomes inflamed as the muscles repair themselves and the tiny tears heal. Your muscles recover within a few days, and the inflammation goes away.
With continued exercise, the muscle tissue tears and rebuilds again and again.
To watch the full episode on Muscle Growth and Hypertrophy, click here for more 👇
TIME STAMPS:
00:00 Intro 00:49 Plugs 02:11 Episode Introduction 06:05 Different types of muscle tissue 07:20 The skeletal muscle structure 11:48 What is hypertrophy? 15:55 How to build muscles and maximize hypertrophy? 18:43 Building muscles: Carbohydrates 20:33 Building muscles: Protein 24:42 Protein recommendations for building muscles 29:32 A Scientific Explanation of how hypertrophy works 34:06 Things you can do to maximize hypertrophy.
In today’s episode, we will talk about ventilators and how they can help healthcare professionals treat patients.
Not every nurse will have a patient on a ventilator or work directly with it, but most emergent situations require one.
It is always good to at least know the basics of a ventilator, so as a nurse, you know how you can use it if a situation arises.
Mechanical Ventilation
Mechanical ventilation is an invasive way to provide oxygen to someone who is unconscious or needs help breathing. This machine is usually seen around ICUs or hospice care settings.
A mechanical ventilator is a machine that assists with oxygenation and directly inflates and deflates the lungs. It is used in a variety of situations like surgery and emergencies.
Ventilator settings are inputs on a machine that determines how much support the patient needs. When we program a ventilator to a specific setting, we account for two things: oxygenation and ventilation.
Ventilation is the process of inhaling and exhaling.
Oxygenation is the process of adding oxygen to the body [1].
Normal inspiration generates negative intrapleural pressure. In return, this creates a pressure gradient between the atmosphere and the alveoli that result in airflow.
In mechanical ventilation, the pressure gradient results from increased (positive) pressure of the air source.
Peak airway pressure
The peak airway pressure is measured at the airway opening and is routinely displayed by mechanical ventilators.
It represents the total pressure needed to push a volume of gas into the lungs and is composed of pressures resulting from inspiratory flow resistance (resistive pressure).
The elastic recoil of the lung and chest wall (elastic pressure), and the alveolar pressure present at the beginning of the breath (positive end-expiratory pressure, PEEP)
Resistive pressure is the pressure from the circuit resistance and airflow. In the mechanically ventilated patient, resistance to airflow occurs in the ventilator circuit, the endotracheal tube, and, most importantly, the patient’s airways.
Elastic pressure
The pressure of the elastic recoil of the lungs and chest wall and the volume of gas delivered. For a given volume, elastic pressure is increased by increased lung stiffness (as in pulmonary fibrosis) or restricted excursion of the chest wall or diaphragm (eg, intense ascites or massive obesity). Because elastance is the inverse of compliance, high elastance is the same as low compliance.
End-expiratory pressure
The end-expiratory pressure In the alveoli usually is the same as atmospheric pressure. However, when the alveoli fail to empty because of airway obstruction. It could be airflow limitation or shortened expiratory time; end-expiratory pressure may be positive relative to the atmosphere.
This pressure is called intrinsic PEEP or autoPEEP to differentiate it from externally applied (therapeutic) PEEP. It is created by adjusting the mechanical ventilator or by placing a tight-fitting mask. This mask applies positive pressure throughout the respiratory cycle.
The pressure is given in the expiratory phase to prevent the closure of the alveoli and allow increased time for O2 exchange.
Used in patients who haven’t responded to treatment and require a high amount of FiO2.
PEEP will lower O2 requirements by recruiting more surface area.
Normal PEEP is approximately 5cmH20. Can be as high as 20cmH20.
Intrinsic PEEP (auto-PEEP)
Intrinsic PEEP or auto-PEEP can be measured in the passive patient through an end-expiratory hold maneuver. Immediately before a breath, the expiratory port is closed for 2 seconds. Flow ceases, eliminating resistive pressure. Thus resulting pressure reflects alveolar pressure at the end of expiration (intrinsic PEEP).
Accurate measurement depends on the patient being completely passive on the ventilator. It is unwarranted to use neuromuscular blockade. Solely to measure intrinsic PEEP.
A non-quantitative method of identifying intrinsic PEEP is to inspect the expiratory flow tracing. Check if the expiratory flow continues until the next breath of the patient. If the patient’s chest fails to come to rest before the next breath, intrinsic PEEP is present.
The consequences of elevated intrinsic PEEP are increased inspiratory work of breathing and decreased venous return. This may result in decreased cardiac output and hypotension.
Airway Management
Airway cuffs
An inflated cuff helps with holding the airway in place
Reduces tidal volume loss
Decreases chance of aspiration
If a patient can speak, makes a weird noise from the cuff, or loses tidal volume, the cuff most likely needs more air.
Ventilator Settings and Modes
When you’re looking at the ventilator screen, it can be a little overwhelming at first. There are a lot of numbers, letters, and words. It is essential to also not change any of those settings if you are unsure about operating it [2].
Ventilator Settings
Tidal volume
The tidal volume is the air moving in and out of the lungs. The average adult breathes about 7 milliliters per kilogram of body weight. For males, the average Vt is 500 ml, and for females, about 400 ml.
Minute ventilation
The amount of volume inhaled and exhaled over 60 seconds. The average range is between 4 and 6 liters.
VE can be increased by taking deeper breaths or increasing the respiratory rate.
Alveolar ventilation
VA is similar to VE but without including dead space. Dead space is the air that is not undergoing active gas exchange.
VA can be increased by breathing harder.
When the volume is too high, there is a risk of overinflation. However, when the volume is too low, it allows atelectasis.
Frequency (Rate)
Respiratory rate is the number of breaths per minute. The average amount of breaths a person takes is 16. The vent can be programmed to deliver x amount of breaths a minute.
FiO2
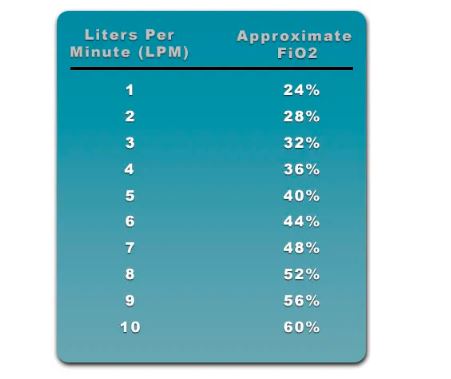
The FiO2, or fraction of inspired oxygen, is the concentration of oxygen that the patient is inhaling.The FiO2 of room air is about 21%. It is good to know that when you use a flow rate of 1, it increases the FiO2 to 24%. For every liter, after that, it increases FiO2 by 4%.
For patients with severe hypoxemia, a FiO2 of 100% may be required when mechanical ventilation is initiated. But your goal should be to wean the FiO2 down to the lowest possible level. That way, it provides adequate oxygenation.
If a patient receives a FiO2 > 60% for a prolonged period, it increases their chances of oxygen toxicity.
Flow Rate
The inspiratory flow rate is a rate that controls how fast a tidal volume is then delivered. The ventilator setting can also adjust depending on the patient’s inspiratory demands.
The average inspiratory flow rate should be set at around 60 L/min. With that said, most ventilators can deliver up to 120 L/min if a patient needs a prolonged expiratory time.
This is necessary when obstructive diseases are present.
If the flow rate is set too low, it could result in patient-ventilator dyssynchrony and an increased work of breathing.
If the flow rate is too high, it could decrease mean airway pressure.
I:E Ratio
The I:E ratio refers to a ratio of the inspiratory portion compared to the expiratory portion of the breathing cycle.
For patients on the ventilator, the normal I:E ratio is between 1:2 and 1:4. A larger I:E ratio may be delivered if a patient is in need of a longer expiratory time. It could be due to the possibility of air trapping.
The I:E ratio can be adjusted by making changes to the flow rate, inspiratory time, expiratory time, tidal volume, and frequency settings.
Sensitivity
The sensitivity control determines how much effort (negative pressure) the patient must generate. This sensitivity can trigger a breath from the machine.
A normal sensitivity setting should be set between -1 and -2 cmH2O. If the sensitivity is set too high, it will cause the ventilator to start auto-triggering.
In return, it will increase the total frequency of breaths. If it’s set too low, the patient could have a difficult time initiating a breath.
Differences between PEEP, Pip, Pplat, and Alarms
PEEP
PEEP is a positive pressure delivered during the expiratory phase of the breathing cycle. It delivers breathing to prevent the closure of alveoli. It also allows increased time for oxygen exchange to occur.
It’s indicated for patients with refractory hypoxemia and those who have not responded well to a high FiO2.
Peak Insp. Pressure (Pip)
Pip is the maximum pressure during inspiration. The goal is to have it under 35, with the goal of preventing lung injury.
Plateau Pressure (Pplat)
Pplat measures lung compliance. This is measured at the end of inspiration with a hold, the goal is to have it under <30.
Alarms
A ventilator alarm is a safety mechanism on a mechanical ventilator. It uses set parameters to provide alerts whenever there is a potential problem. This problem could be related to the patient-ventilator interaction.
High Pressure
Low Pressure
Low Expired Volume
High Frequency
Apnea
High PEEP
Low PEEP
Primary Control and Modes
In mechanical ventilation, there are two primary control variables [3]:
1. Volume Control
Volume Control means that you can set (or control) the patient’s tidal volume.
So with a set tidal volume and a set respiratory rate, this means that there is minute ventilation.
This is good when it comes to making adjustments to achieve the desired PaCO2.
The cons of using Volume Control are that the tidal volume is preset, and a patient’s lung is weak. It can result in high peak pressures.
Another drawback of Volume Control is patient-ventilator dyssynchrony.
2. Pressure Control
Pressure Control means that you can set (or control) the patient’s pressure to achieve a desired tidal volume.
As with Volume Control, a Pressure-Controlled tidal volume and set rate can help you reach the desired PaCO2.
The main disadvantage of using pressure control is the patient’s tidal volume. It can be unstable if there are changes in the patient’s lung compliance or airway resistance.
Volume Control and Pressure Control — are the two control variables. When initiating mechanical ventilation on a patient. Once you select the control variable, you can now choose the actual operational mode. It will determine the pattern of breathing for the patient.
Assist/Control (A/C) Mode
In this mode, the smallest number of preset mandatory breaths is delivered by the ventilator.
However, the patient can also trigger assisted breaths. The patient makes an effort to breathe, and the ventilator assists in delivering it.
With that said, this mode of ventilation does not allow the patient to take spontaneous breaths. In this mode, the operator can set either a controlled pressure or a controlled volume.
The sensitivity control can also be adjusted to make it easier or harder for the patient to start a breath.
When to use a Ventilator
This mode is most often used when mechanical ventilation is first initiated for a patient. It provides full ventilatory support for the patient.
One of the advantages of using Assist/Control is that it keeps the patient’s breathing needs very low.
One of the major complications of Assist/Control is hyperventilation. This complication results in respiratory alkalosis. It is also the result when the patient has too many breaths. This is whether patient-triggered or machine-triggered.
In this mode, the ventilator delivers a preset small number of mandatory breaths. But it also allows the patient to start spontaneous breaths between the mandatory breaths.
This mode also allows the operator to set either a controlled pressure or a controlled volume.
When to Use SIMV?
The primary sign of SIMV is when a patient needs partial ventilatory support. Since the patient can now take spontaneous breaths, they can also contribute to some of their minute ventilation. SIMV is a mode that is often used for weaning as well.
Advantages of Using SIMV
Because the patient can do spontaneous breaths, their respiratory muscle strength returned. It also helps the patient avoid muscular atrophy.
It distributes tidal volumes throughout the lung fields, which reduces V/Q mismatching. Besides that, it also helps to decrease the patient’s mean airway pressure.
To catch up on the full episode of Ep. 158, click here for more 👇
TIMESTAMPS:
00:00 Intro 00:45 Plugs 02:04 Podcast Introduction 04:19 When is Mechanical Ventilation Needed? 07:59 Respiratory Mechanics 10:14 Peak Airway Pressure 12:41 End-expiratory pressure 13:31 Intrinsic PEEP (auto-PEEP) 15:21 Air management Tips 17:42 Mode & Settings: Tidal Volume Mode 21:56 Mode & Settings: Frequency (Rate) 22:59 Mode & Settings: FiO2 – Fraction of Inspired Oxygen 26:27 Mode & Settings: Flow Rate 27:53 Mode & Settings: I:E Ratio 30:12 Mode & Settings: Sensitivity 32:27 Mode & Settings: PEEP 34:51 Primary Control and Modes: Volume Control 37:13 Primary Control and Modes: Pressure Control 38:23 Primary Control and Modes: Assist/Control (A/C) Mode 39:23 Primary Control and Modes: Synchronous Intermittent Mandatory Ventilation (SIMV) 42:56 Learn the basics 45:45 Dealing with ventilator alarms 46:28 Criteria for weaning off the ventilator 54:16 Wrapping up the episode





Recent Comments